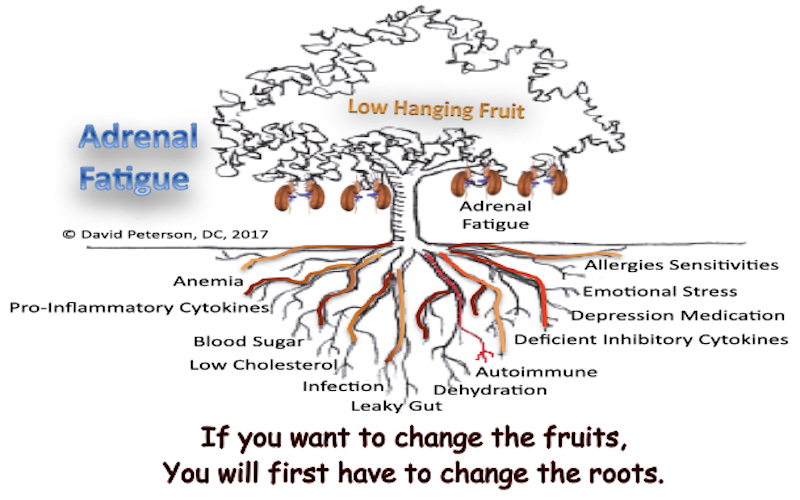
Adrenal dysfunction is not a primary diagnosis—it is a symptom of deeper physiological dysfunction. Conventional protocols often rely on oversimplified models that treat adrenal fatigue as an isolated disorder. However, adrenal imbalance is always secondary to broader systemic issues that must be addressed first. If these underlying dysfunctions remain unresolved, any attempt at adrenal rehabilitation will be temporary and ineffective.
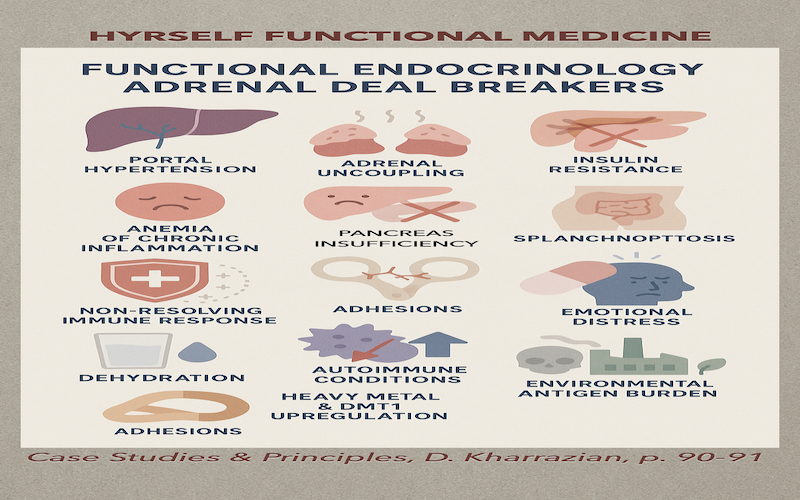
We’re breaking down the underlying causes of adrenal dysfunction presented by Dr. Kharrazian at the “Case Studies and Principles” seminar, where he discussed the critical factors you must address first, and why skipping these steps could sabotage your recovery. In this article, we explore the most critical adrenal deal breakers—the physiological mechanisms that disrupt, delay, or entirely block adrenal recovery.
- Portal Hypertension: The Hidden Vascular Burden
- Adrenal Uncoupling: Mitochondrial Chaos
- Anemia: The Oxygen Deficit No One Talks About
- Insulin Resistance: The Endocrine Saboteur
- Low Cholesterol: The Steroid Precursor Deficiency
- Non-Resolving Immune Responses: The Fire That Won’t Go Out
- Splanchnoptosis: The Fallen Organs Syndrome
- Surgical Menopause: Hormonal Shockwave
- Dehydration: The Forgotten Stressor
- Adhesions: Fascia that Chokes the Flow
- Chronic SSRI Usage: Flattened Stress Response
- Emotional Stress: The Trigger and the Fuel
- Autoimmune Conditions: Self-Attack on Endocrine Tissue
- Heavy Metals & DMT1 Upregulation: The Inflammatory Loop
- Environmental Antigen Burden: Modern Toxicity Overload
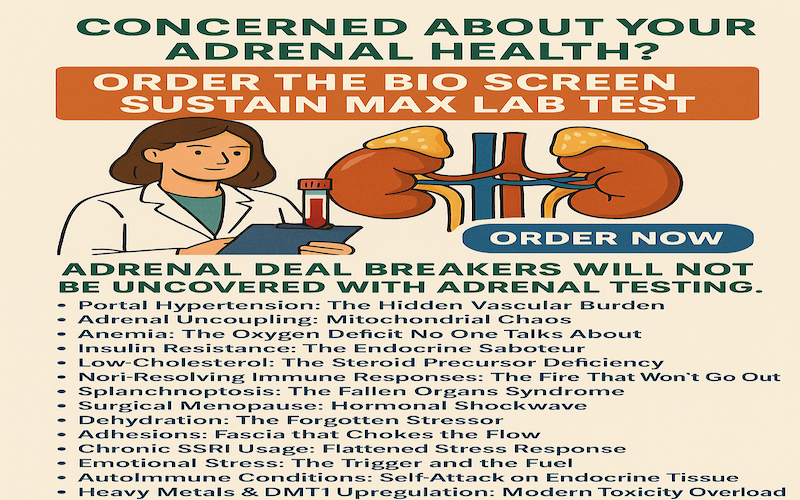
Sick and Tired of Being Sick and Tired?
Adrenal Testing will not reveal any of the Adrenal Fatigue Deal Breakers. Get the clarity your health deserves with the BioScreen Sustain Max blood test.
Whether you’re just beginning your wellness journey or following up on previous results, this advanced panel provides in-depth insight into your body’s most critical systems—far beyond standard Adrenal lab tests.
What’s Included:
✅ Blood sugar & insulin function
✅ Cardiovascular and lipid health
✅ Hidden infections and inflammation
✅ Thyroid performance
✅ Anemia and electrolyte balance
✅ Liver and bile function
✅ Urinalysis with 13 key markers
Total: 61 biomarkers + 13 urinalysis evaluations—all in one comprehensive screen.
🔬 Take control of your health now.
Click below to order your BioScreen Sustain Max and start uncovering the hidden reasons behind your fatigue, inflammation, or stubborn symptoms.
👉 BioScreen Sustain Max and move from guessing… to knowing.
Understanding the Root: Why Simplified Adrenal Protocols Fail
Adrenal fatigue protocols that rely on supplements like licorice, ashwagandha, or glandulars often mask symptoms without addressing the root dysfunction. These short-term strategies fail when upstream mechanisms like chronic inflammation, immune dysregulation, or impaired hepatic function are active.
The following are non-negotiable physiological barriers that must be investigated and treated to restore genuine adrenal function.
1. Portal Hypertension: The Hidden Vascular Burden
Portal hypertension—elevated blood volume in the portal venous system bypassing the liver, impairs hepatic detoxification, and promotes systemic inflammation. The result is a recirculation of toxic metabolites that place sustained stress on the HPA axis (hypothalamic-pituitary-adrenal). This stress reduces adrenal resilience, suppresses cortisol metabolism, and perpetuates fatigue.

Key Indicators:
- Elevated AST/ALT > 26 with normal imaging.
- High Blood Pressure | Prescription for High Blood Pressure
- Esophageal varices or GI bleeding distorting Lower Esophageal Sphincter causing symptoms of Acid Reflux and GERD.
- Internal or External Hemorrhoids. Blooding with bowel movements.
- Elevated ammonia or urea
- Varicose Veins
- Swollen legs/ankles
Recommended Test: 👉 BioScreen Sustain Max and move from guessing… to knowing.
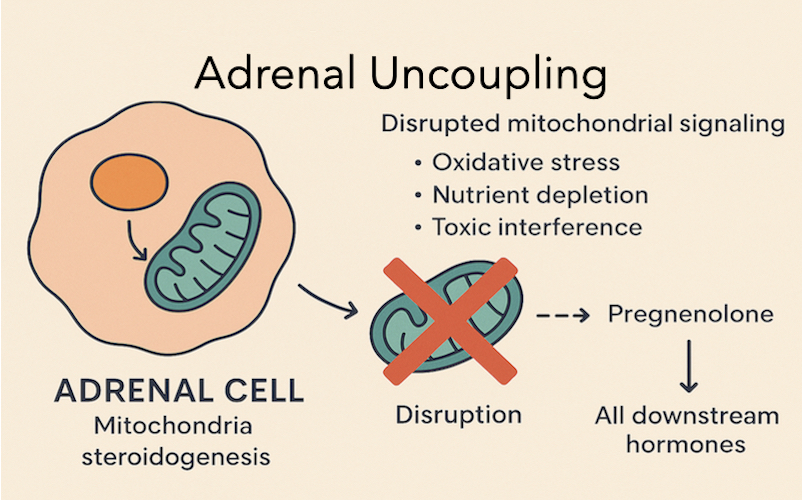
2. Adrenal Uncoupling: Mitochondrial Chaos
Adrenal cells rely heavily on mitochondria for steroidogenesis. Adrenal uncoupling occurs when mitochondrial signaling is disrupted by oxidative stress, nutrient depletion, or toxic interference. This disrupts the conversion of cholesterol into pregnenolone, and thereby all downstream hormones.
Mitochondria are the primary energy producers in the cell through cellular respiration, a process requiring both glucose and oxygen.
How it works:
- Glucose is broken down through a series of steps (including glycolysis and the citric acid cycle) to produce energy in the form of ATP (adenosine triphosphate).
- Oxygen acts as the final electron acceptor in the electron transport chain, a crucial step in ATP production.
- Without both glucose and oxygen, mitochondria cannot efficiently produce ATP, hindering the cell’s ability to perform vital functions.



Insulin resistance and disturbed delivery:
Insulin resistance affects the body’s ability to utilize glucose efficiently.
- Insulin promotes glucose uptake into cells, particularly in tissues like muscle, fat, and liver, so it can be used for energy or storage.
- In insulin resistance, cells don’t respond properly to insulin, leading to impaired glucose uptake and utilization.
- This can result in higher blood glucose levels (hyperglycemia), as the body struggles to get glucose into the cells that need it.
- While insulin’s direct effect on mitochondrial function is still being investigated, research suggests that insulin resistance can lead to mitochondrial dysfunction in various tissues, including muscle and liver.
- Mitochondrial dysfunction in insulin resistance may include reduced ATP production and increased production of reactive oxygen species (ROS), further impairing insulin signaling and potentially contributing to metabolic complications.
Therefore, insulin resistance can directly disrupt the “delivery” of glucose to the mitochondria by hindering glucose uptake into cells, thus impacting their energy production capabilities.
Common Causes:
- Insulin Resistance
- Mitochondrial dysfunction from chronic infections
- Glyphosate and EMF exposure
- Persistent oxidative load
Recommended Test: 👉 BioScreen Sustain Max and move from guessing… to knowing.
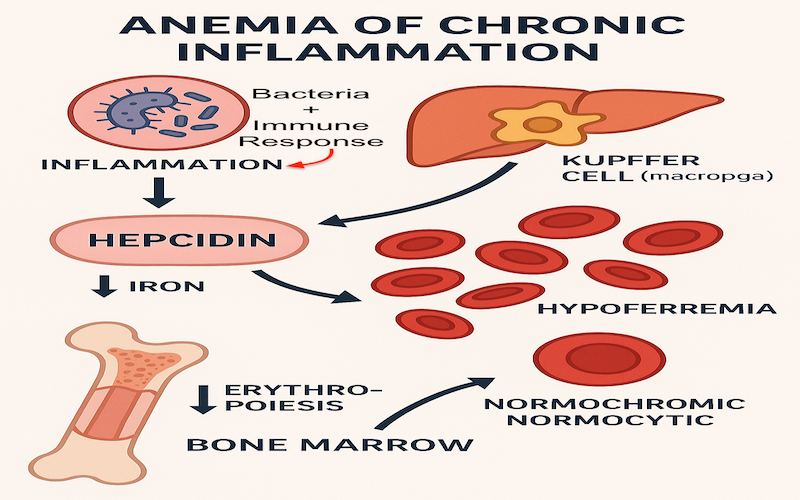
3. Anemia: The Oxygen Deficit No One Talks About

Adrenals require oxygen-rich blood to produce hormones. Anemia—particularly Anemia of Chronic Inflammation (which causes LOW IRON LEVELS), Hyperferitinemia due to non-resolving inflammation, Covid Vaccines, or Alkaline ph — reduces oxygen delivery to adrenal tissues, limiting energy production and hormone output.
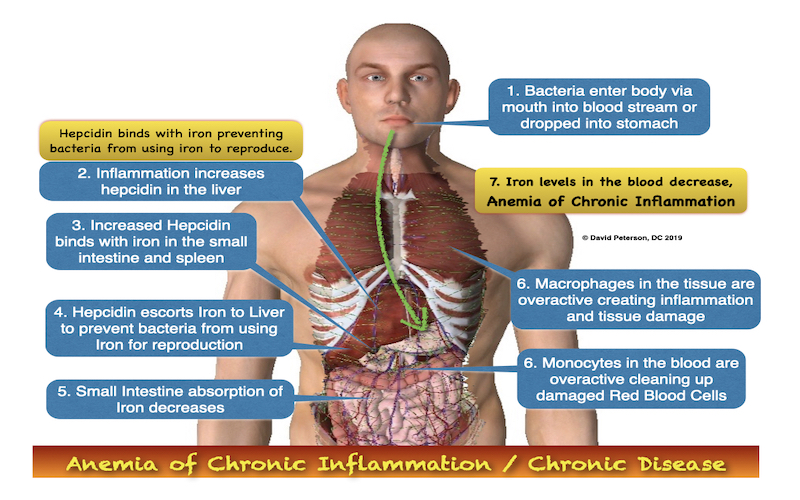
Anemia of Chronic Disease (ACD), also known as anemia of inflammation or hypoferremia of inflammation, is a type of anemia often seen in people with ongoing health issues—such as infections, autoimmune diseases, cancer, or other long-term illnesses like diabetes or trauma. It’s also more common in older adults or anyone with chronic immune system activation.
Watch For:
- Fatigue unrelieved by rest
- Low serum ferritin, MCV, or hemoglobin
- Cold extremities and shortness of breath
Recommended Test: 👉 BioScreen Sustain Max and move from guessing… to knowing.
4. Insulin Resistance: The Endocrine Saboteur
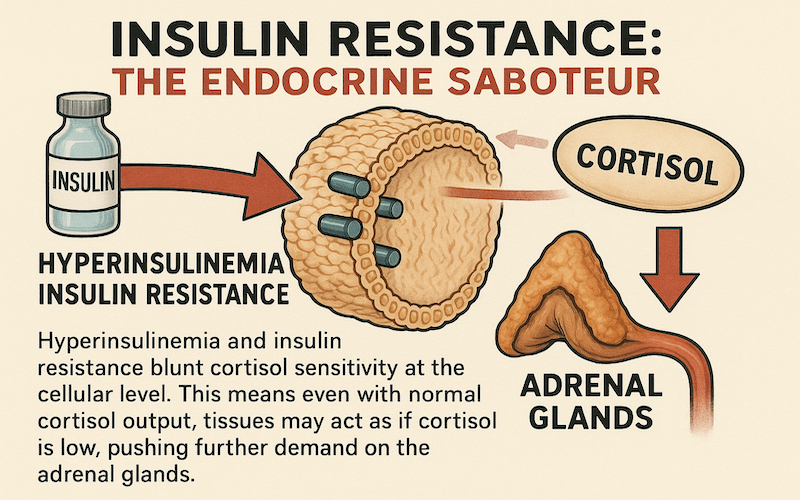
Hyperinsulinemia and insulin resistance blunt cortisol sensitivity at the cellular level. This means even with normal cortisol output, tissues may act as if cortisol is low, pushing further demand on the adrenal glands.
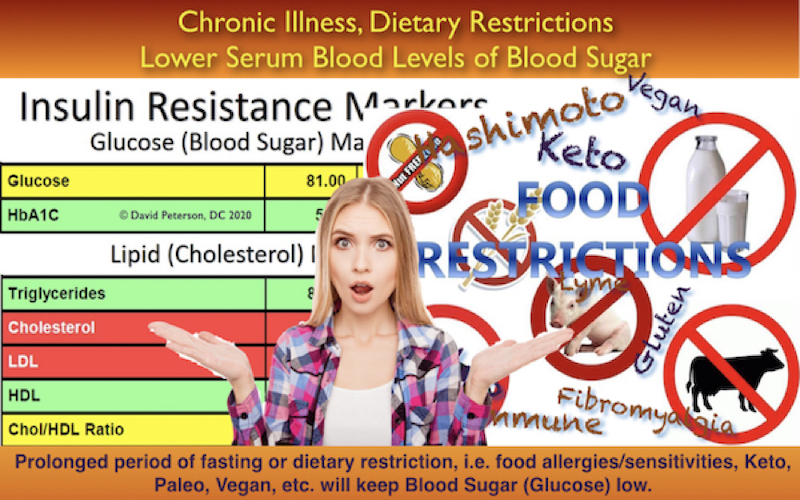
Metabolic Warning Signs:
- High Cholesterol, Triglycerides, LDL, Cholesterol/HDL ratio >3.1, with normal or high glucose
- Abdominal weight gain
- Fasting insulin above 7 μIU/mL
- Post-meal fatigue or sugar cravings
Recommended Test: 👉 BioScreen Sustain Max and move from guessing… to knowing.
5. Low Cholesterol: The Steroid Precursor Deficiency
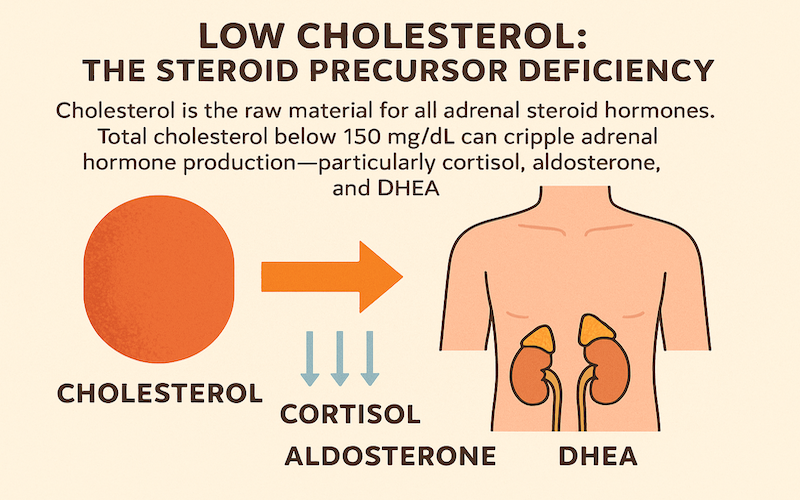
Cholesterol is the raw material and necessary building block for all adrenal steroid hormones. Every hormone is built from a cholesterol molecule. Total cholesterol below 150 mg/dL can cripple adrenal hormone production—particularly cortisol, aldosterone, and DHEA.
Low Cholesterol Triggers:
- Vegan/low-fat diets
- Statin medications
- Chronic malabsorption or liver dysfunction
Recommended Test: 👉 BioScreen Sustain Max and move from guessing… to knowing.
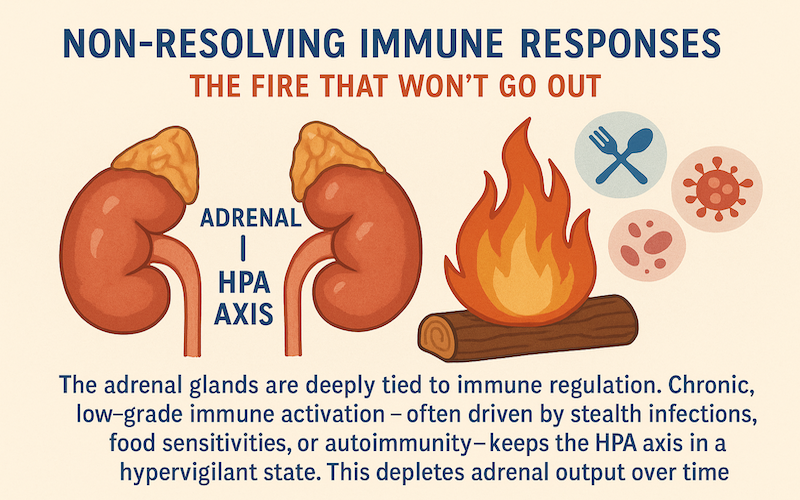
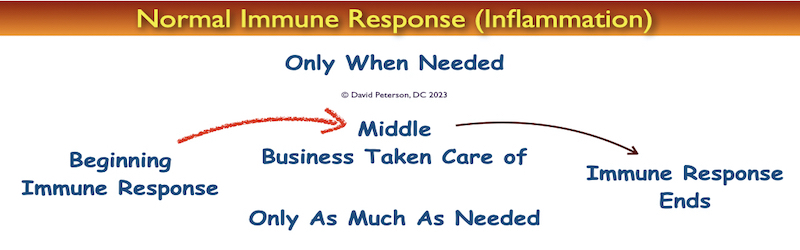
6. Non-Resolving Immune Responses: The Fire That Won’t Go Out
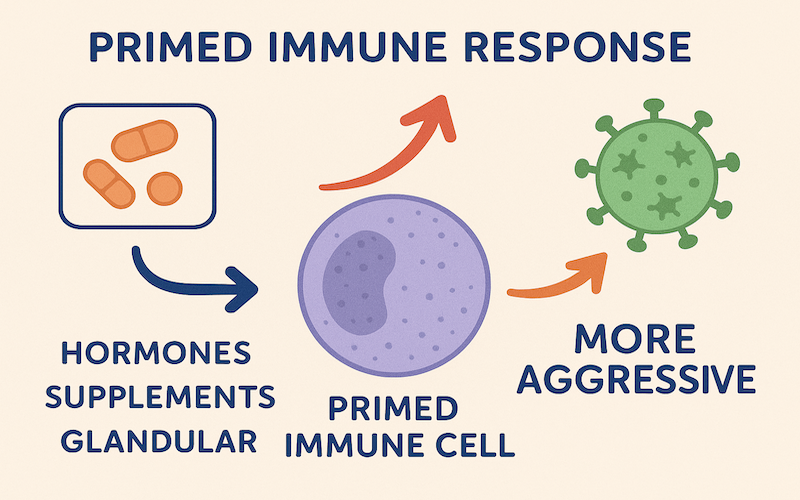
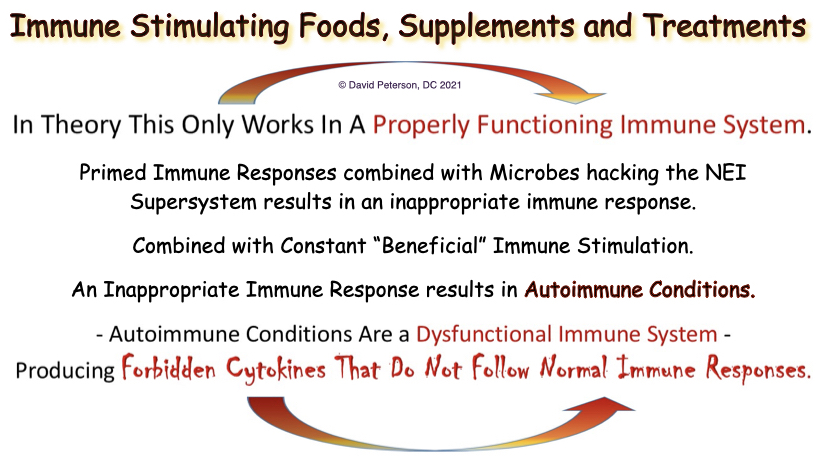
The adrenal glands are deeply tied to immune regulation. Chronic, low-grade immune activation—often driven by a sterile inflammation, constant use of immune boosting, stimulating and strengthening supplements, or immune stimulating estradiol hormone replacement—keeps the HPA axis in a hypervigilant state. This depletes adrenal output over time.
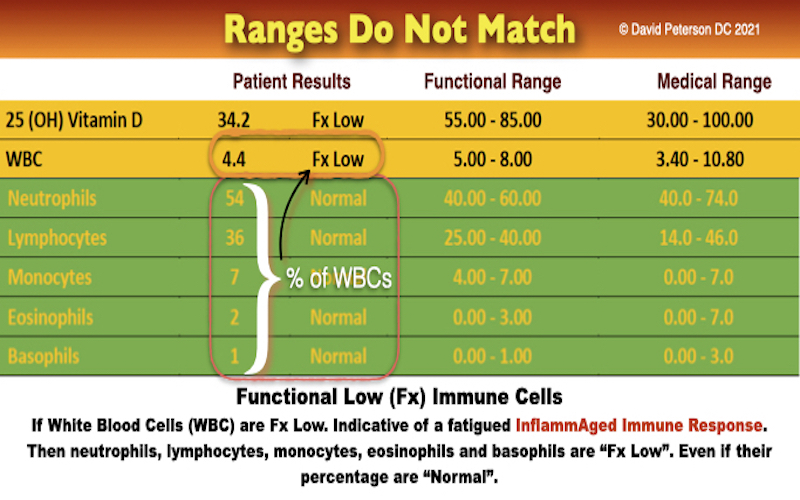
Inflammaged Immune Response
Inflammaging, which has been described as a state of low-grade chronic inflammation associated with dysfunctional immunity, is the hallmark of immunosenescence. The consequences of both processes may lead to increased susceptibility to infection and poor responses to vaccination as well as to chronic inflammatory and degenerative diseases.
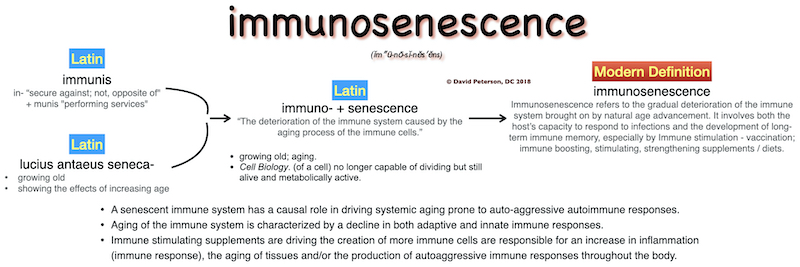
Infection in the body and the interactions between the immune response and microbe/antigen set the stage for a “Fertile Field” where the body and/or target organ is “Primed” for subsequent disease.1Fujinami RS, von Herrath MG, Christen U, Whitton JL. Molecular mimicry, bystander activation, or viral persistence: infections and autoimmune disease. Clin Microbiol Rev. 2006;19(1):80-94. doi:10.1128/CMR.19.1.80-94.2006 Long-term immune stimulation prematurely ages the immune system, creates a primed immune response and leads to the progression of disease.2Valenzuela HF, Effros RB. Divergent telomerase and CD28 expression patterns in human CD4 and CD8 T cells following repeated encounters with the same antigenic stimulus. Clin Immunol 2002;105:117–125.,3Vallejo AN. CD28 extinction in human T cells: altered functions and the program of T-cell senescence. Immunol Rev 2005;205:158–169.,4Weng NP, Akbar AN, Goronzy J. CD28(−) T cells: Their role in the age-associated decline of immune function. Trends Immunol 2009;30:306–312.,5Lindstrom TM, Robinson WH. Rheumatoid arthritis: a role for immunosenescence?. J Am Geriatr Soc. 2010;58(8):1565-1575. doi:10.1111/j.1532-5415.2010.02965.x Individuals with Autoimmune conditions are immunocompromised,6Baecklund E, Iliadou A, Askling J, et al. Association of chronic inflammation, not its treatment, with increased lymphoma risk in rheumatoid arthritis. Arthritis Rheum 2006;54:692–701.,7Doran MF, Crowson CS, Pond GR, et al. Frequency of infection in patients with rheumatoid arthritis compared with controls: A population-based study. Arthritis Rheum 2002;46:2287–2293. and accumulating evidence suggests that premature aging of the immune system contributes to the development of autoimmune conditions.8Colmegna I, Diaz-Borjon A, Fujii H, et al. Defective proliferative capacity and accelerated telomeric loss of hematopoietic progenitor cells in rheumatoid arthritis. Arthritis Rheum 2008;58:990–1000.,9Koetz K, Bryl E, Spickschen K, et al. T cell homeostasis in patients with rheumatoid arthritis. Proc Natl Acad Sci U S A 2000;97:9203–9208.,10Schmidt D, Goronzy JJ, Weyand CM. CD4+ CD7− CD28− T cells are expanded in rheumatoid arthritis and are characterized by autoreactivity. J Clin Invest 1996;97:2027–2037.,11Wagner UG, Koetz K, Weyand CM, et al. Perturbation of the T cell repertoire in rheumatoid arthritis. Proc Natl Acad Sci U S A 1998;95:14447–14452.
Suspect This When:
- White Blood Cells Low with Normal Percentages of Neutrophils, Lymphocytes, Monocytes, Eosinophils, and Basophils.
- CRP or ESR is persistently elevated
- Antibody levels remain high post-infection
- Food intolerance testing shows broad reactivity
Recommended Test: 👉 BioScreen Sustain Max and move from guessing… to knowing.
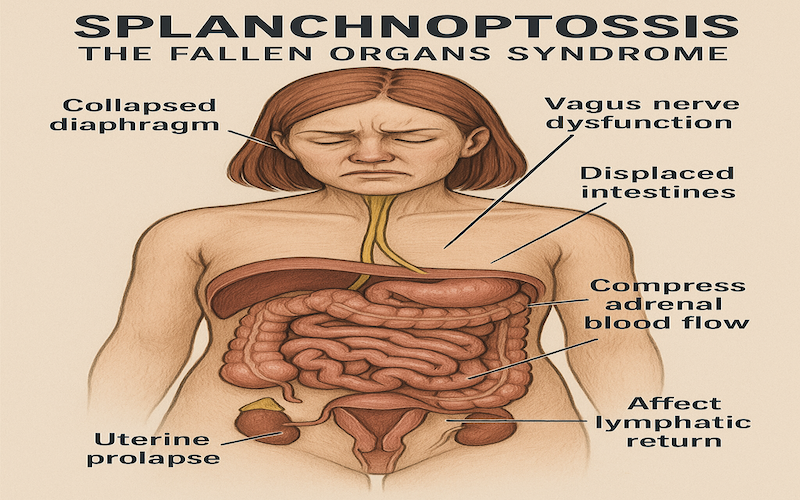
7. Splanchnoptosis: The Fallen Organs Syndrome
Splanchnoptosis, or visceral prolapse, causes mechanical stress on the abdominal organs. A dropped kidney, displaced intestines, or uterine prolapse may trigger Vasomotor dysfunction, distrubing adrenal blood flow, or affect lymphatic return—all of which compromise adrenal stability.
Symptoms Include:
- Bloating and early satiety
- Diaphragmatic breathing difficulty
- Pelvic heaviness or uterine tilt
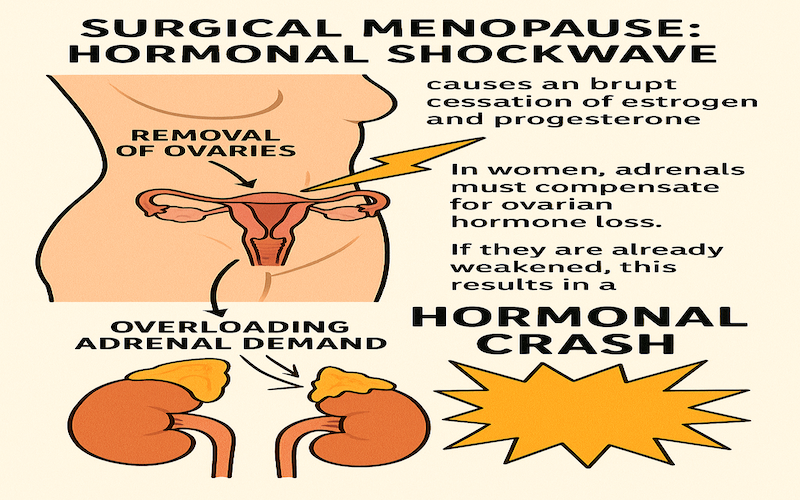
8. Surgical Menopause: Hormonal Shockwave
Removal of ovaries (oophorectomy) causes an abrupt cessation of estrogen and progesterone, overloading adrenal demand. In women, adrenals must compensate for ovarian hormone loss. If they are already weakened by the other Adrenal Deal Breakers, this results in a hormonal crash.
Expect:
- Rapid onset of insomnia, anxiety, and hot flashes
- Loss of resilience to stress
- Skyrocketing FSH/LH with low DHEA
9. Dehydration: The Forgotten Stressor
Even mild dehydration increases vasopressin and aldosterone demand, burdening the adrenal cortex. Low water intake, high caffeine use, or excessive sweating can silently deplete adrenal resources.
Early Signs:
- Dark urine and dry lips
- Orthostatic hypotension
- Salt cravings
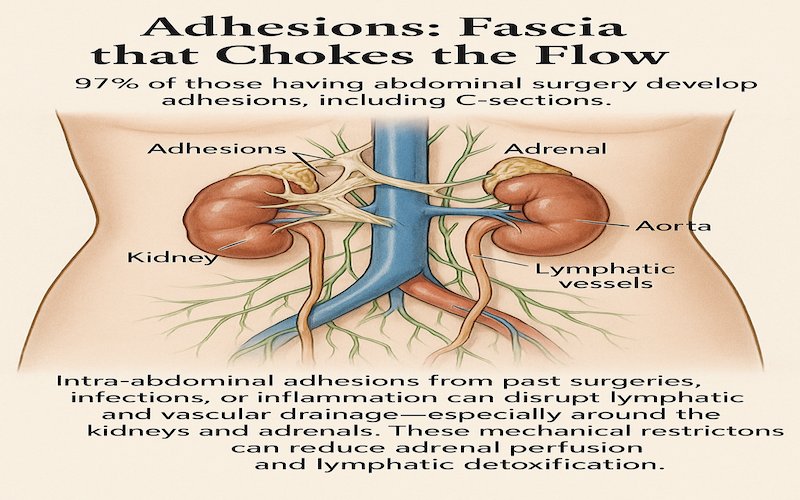
10. Adhesions: Fascia that Chokes the Flow
Intra-abdominal adhesions from past surgeries, infections, or inflammation can disrupt lymphatic and vascular drainage—especially around the kidneys and adrenals. 93% of individuals, who have undergone surgery develop adhesions that limit the mobility and movement of abdominal organs, leading to impaired organ function and disrupted blood flow. These mechanical restrictions can reduce adrenal perfusion and lymphatic detoxification.
Consider This With:
- Surgical history (Gallbladder, Appendix, C-section, hysterectomy, etc.)
- Chronic pelvic or abdominal pain
- Failed response to adrenal support
11. Chronic SSRI Usage: Flattened Stress Response
The hypothalamus and adrenal glands play a vital role in the body’s stress response, especially in situations of social defeat. The hypothalamus coordinates behavioral and physiological reactions by activating neural circuits involved in defense and social behavior. Simultaneously, the adrenal glands release stress hormones that prime the body for action. Chronic social stress can alter both hypothalamic and adrenal function, disrupting HPA axis regulation and leading to imbalanced hormone output over time.
SSRIs can blunt cortisol signaling and suppress ACTH release, weakening the adrenal response over time. While they reduce symptoms of anxiety and depression, they may also mask HPA axis failure.
Selective serotonin reuptake inhibitors (SSRIs) can dampen cortisol signaling and suppress ACTH production, gradually weakening the adrenal response. Although these medications are effective at easing symptoms of anxiety and depression, they may also conceal underlying dysfunction of the HPA (hypothalamic-pituitary-adrenal) axis.
Clinical Clues:
- Flat salivary cortisol curve
- Dependence on medication for mood regulation
- Worsening fatigue over time despite therapy
12. Emotional Stress: The Trigger and the Fuel
Emotional trauma is a primary disruptor of adrenal health, especially in unresolved or repressed forms. The limbic system maintains chronic sympathetic tone, draining adrenal output daily.
High-Risk Indicators:
- History of PTSD, abuse, or loss
- Reactive blood pressure or heart rate
- Somatic body memory symptoms
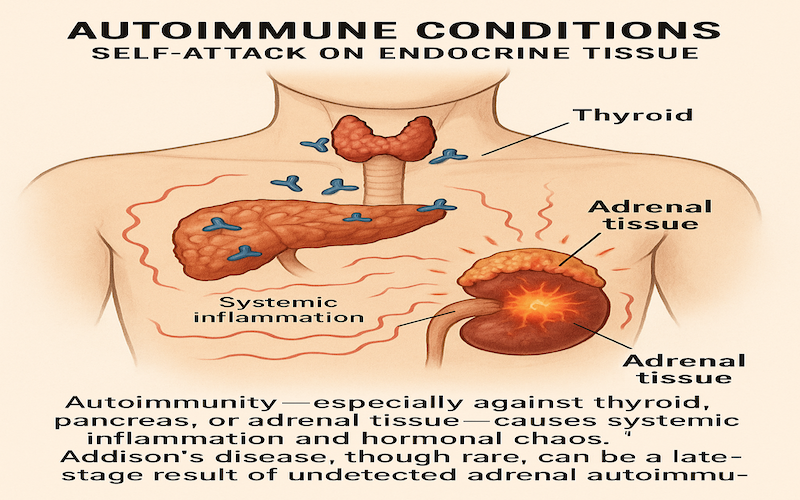
13. Autoimmune Conditions: Self-Attack on Endocrine Tissue
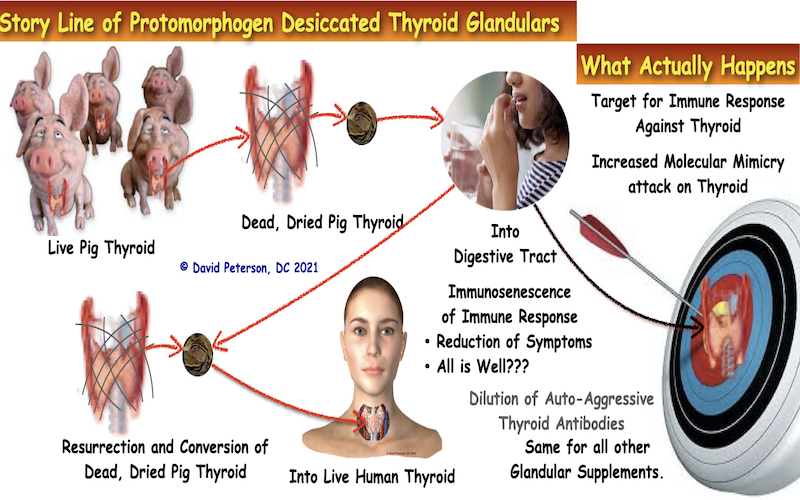
Autoimmunity—especially against thyroid, pancreas, or adrenal tissue—causes systemic inflammation and hormonal chaos. Endocrine glandular supplements can provoke immune responses, but the information is complex and requires careful consideration.
Endocrine glandular supplements and drugs can provoke immune responses in some cases. Here’s a brief explanation:
- Glandular Supplements: These are derived from animal glands (e.g., thyroid, adrenal, or pituitary) and may contain hormones or bioactive compounds. Since they introduce foreign proteins or peptides into the body, they can trigger immune reactions, such as allergic responses or autoimmune activity, especially if the body recognizes these substances as non-self. Contamination or improper dosing can increase this risk.
- Endocrine Drugs: Synthetic or bioidentical hormones (e.g., corticosteroids, thyroid hormones, insulin, or growth hormone) can alter immune function. For example:
- Corticosteroids (like prednisone) suppress immune responses, increasing infection risk.
- Thyroid drugs (like levothyroxine) may rarely cause hypersensitivity reactions.
- Growth hormone or sex hormones (e.g., estrogen or testosterone) modulate immune activity, exacerbating autoimmune conditions like lupus or rheumatoid arthritis in susceptible individuals.
The likelihood and severity of immune responses depend on the specific substance, dosage, underlying health conditions, and individual factors like how primed the immune system is, or pre-existing non-resolving immune “autoimmune” disorders. Always consult a healthcare provider before using such supplements or drugs, as they carry risks of adverse effects, including immune-related complications.
If you have a specific supplement or drug in mind or want details on a particular immune response, let me know, and I can dive deeper!
Trackable Signs:
- Positive ANA, TPO, or adrenal antibodies
- Hypoglycemia with normal insulin
- Episodes of adrenal crisis
14. Heavy Metals & DMT1 Upregulation: The Inflammatory Loop
The DMT1 and other divalent metal transporters function to transport iron into the body so it can be used to make red blood cells. But inflammation stimulates the divalent metal transporters. Inflammation upregulates DMT1, increasing intestinal absorption of toxic metals like mercury, lead, and cadmium. These metals disrupt mitochondrial function in adrenal tissue and block normal enzyme cascades.
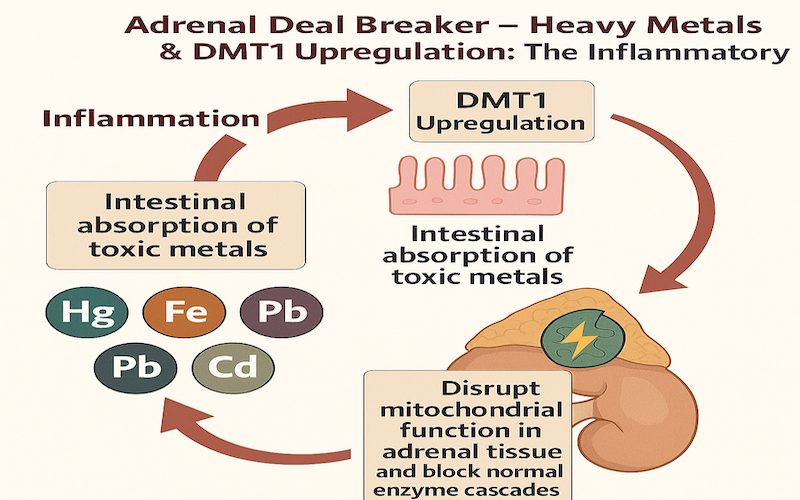
If there is no iron around, DMT1 will start transporting heavy metals in this order: iron Fe(2+), zinc Zn(2+), manganese Mn(2+), copper Cu(2+), cadmium Cd(2+), cobalt Co(2+), nickel Ni(2+), and lead Pb(2+), and mercury Hg(2+).

Toxic elements such as cadmium, mercury and lead share the same iron transporters in the body, and it may be the reason that iron deficiency or Anemia of Chronic Inflammation predisposes humans to cadmium, mercury and lead toxicity.12Park JD, Cherrington NJ, Klaassen CD. Intestinal absorption of cadmium is associated with divalent metal transporter 1 in rats. Toxicol Sci. 2002 Aug;68(2):288-94. doi: 10.1093/toxsci/68.2.288. PMID: 12151624.,13Bressler JP, Olivi L, Cheong JH, Kim Y, Bannona D. Divalent metal transporter 1 in lead and cadmium transport. Ann N Y Acad Sci. 2004 Mar;1012:142-52. doi: 10.1196/annals.1306.011. PMID: 15105261.,14Suzuki T, Momoi K, Hosoyamada M, Kimura M, Shibasaki T. Normal cadmium uptake in microcytic anemia mk/mk mice suggests that DMT1 is not the only cadmium transporter in vivo. Toxicol Appl Pharmacol. 2008 Mar 15;227(3):462-7. doi: 10.1016/j.taap.2007.10.026. Epub 2007 Nov 17. PMID: 18076961.,15Himeno S, Yanagiya T, Enomoto S, Kondo Y, Imura N. Cellular cadmium uptake mediated by the transport system for manganese. Tohoku J Exp Med. 2002 Jan;196(1):43-50. doi: 10.1620/tjem.196.43. PMID: 12498325.Toxic elements can “piggy back” on divalent metal transporters (DMT1)16Mims MP, Prchal JT. Divalent metal transporter 1. Hematology. 2005 Aug;10(4):339-45. doi: 10.1080/10245330500093419. PMID: 16085548. and the other homeostatic mechanisms for iron regulation and can pose a second adverse consequence for the patient with either extremely high iron stores or the patient with iron deficiency, which more often than not is Anemia of Chronic Inflammation.
Warning Symptoms:
- Brain fog and limb numbness
- Strange body odors or metallic taste
- Positive heavy metal panels
15. Environmental Antigen Burden: Modern Toxicity Overload
We live in an antigen-rich environment: mold, VOCs, pesticides, plastics, perfumes. In individuals with a Primed immune response, exposure to substances like mold, VOCs, pesticides, plastics, and perfumes can indeed promote mast cell activation. These disrupt the immune system, increase adrenal demand, and promote mast cell activation, which drives fatigue, insomnia, and histamine overload.
Here’s why:
- Mast cells are a type of immune cell that plays a key role in protecting the body from harm.
- When they encounter triggers, such as foreign substances (xenobiotics) like chemicals or toxins, they release inflammatory chemicals, including histamine, to combat the threat.
- In individuals with Mast Cell Activation Syndrome (MCAS), these mast cells are overly reactive and can release excessive amounts of these chemicals even in response to seemingly harmless substances.
- Exposure to things like mold, VOCs, pesticides, plastics (like BPA), and fragrances can trigger mast cell activation.
- For example, mold toxins (mycotoxins) can directly stimulate mast cells, leading to a release of histamine and other inflammatory molecules.
- Similarly, VOCs, released from various products including new furniture and building materials, can also trigger mast cell activation.
- This excessive release of inflammatory mediators can lead to a wide range of symptoms affecting multiple organs and systems, such as fatigue, respiratory issues, headaches, skin reactions, and digestive problems.
- Chronic exposure to these triggers can lead to a persistent state of inflammation and contribute to the ongoing symptoms of MCAS.
In essence, these environmental triggers can contribute to a hyperactive immune response in sensitized individuals, causing mast cells to become overly reactive and release inflammatory mediators, leading to various symptoms associated with mast cell activation.
Common Clues:
- Reactions to smells, foods, or weather
- Histamine intolerance symptoms
- Multiple chemical sensitivity
Final Thoughts: Investigate Before You Supplement
Adrenal dysfunction is never isolated. Any attempt at adrenal support must include a complete physiological map. Evaluate root-cause barriers before prescribing adaptogens or glandulars. The above deal breakers are common, often silent, and always significant.
References
- 1Fujinami RS, von Herrath MG, Christen U, Whitton JL. Molecular mimicry, bystander activation, or viral persistence: infections and autoimmune disease. Clin Microbiol Rev. 2006;19(1):80-94. doi:10.1128/CMR.19.1.80-94.2006
- 2Valenzuela HF, Effros RB. Divergent telomerase and CD28 expression patterns in human CD4 and CD8 T cells following repeated encounters with the same antigenic stimulus. Clin Immunol 2002;105:117–125.
- 3Vallejo AN. CD28 extinction in human T cells: altered functions and the program of T-cell senescence. Immunol Rev 2005;205:158–169.
- 4Weng NP, Akbar AN, Goronzy J. CD28(−) T cells: Their role in the age-associated decline of immune function. Trends Immunol 2009;30:306–312.
- 5Lindstrom TM, Robinson WH. Rheumatoid arthritis: a role for immunosenescence?. J Am Geriatr Soc. 2010;58(8):1565-1575. doi:10.1111/j.1532-5415.2010.02965.x
- 6Baecklund E, Iliadou A, Askling J, et al. Association of chronic inflammation, not its treatment, with increased lymphoma risk in rheumatoid arthritis. Arthritis Rheum 2006;54:692–701.
- 7Doran MF, Crowson CS, Pond GR, et al. Frequency of infection in patients with rheumatoid arthritis compared with controls: A population-based study. Arthritis Rheum 2002;46:2287–2293.
- 8Colmegna I, Diaz-Borjon A, Fujii H, et al. Defective proliferative capacity and accelerated telomeric loss of hematopoietic progenitor cells in rheumatoid arthritis. Arthritis Rheum 2008;58:990–1000.
- 9Koetz K, Bryl E, Spickschen K, et al. T cell homeostasis in patients with rheumatoid arthritis. Proc Natl Acad Sci U S A 2000;97:9203–9208.
- 10Schmidt D, Goronzy JJ, Weyand CM. CD4+ CD7− CD28− T cells are expanded in rheumatoid arthritis and are characterized by autoreactivity. J Clin Invest 1996;97:2027–2037.
- 11Wagner UG, Koetz K, Weyand CM, et al. Perturbation of the T cell repertoire in rheumatoid arthritis. Proc Natl Acad Sci U S A 1998;95:14447–14452.
- 12Park JD, Cherrington NJ, Klaassen CD. Intestinal absorption of cadmium is associated with divalent metal transporter 1 in rats. Toxicol Sci. 2002 Aug;68(2):288-94. doi: 10.1093/toxsci/68.2.288. PMID: 12151624.
- 13Bressler JP, Olivi L, Cheong JH, Kim Y, Bannona D. Divalent metal transporter 1 in lead and cadmium transport. Ann N Y Acad Sci. 2004 Mar;1012:142-52. doi: 10.1196/annals.1306.011. PMID: 15105261.
- 14Suzuki T, Momoi K, Hosoyamada M, Kimura M, Shibasaki T. Normal cadmium uptake in microcytic anemia mk/mk mice suggests that DMT1 is not the only cadmium transporter in vivo. Toxicol Appl Pharmacol. 2008 Mar 15;227(3):462-7. doi: 10.1016/j.taap.2007.10.026. Epub 2007 Nov 17. PMID: 18076961
- 15Himeno S, Yanagiya T, Enomoto S, Kondo Y, Imura N. Cellular cadmium uptake mediated by the transport system for manganese. Tohoku J Exp Med. 2002 Jan;196(1):43-50. doi: 10.1620/tjem.196.43. PMID: 12498325.
- 16Mims MP, Prchal JT. Divalent metal transporter 1. Hematology. 2005 Aug;10(4):339-45. doi: 10.1080/10245330500093419. PMID: 16085548.