Explore the intriguing Wolff–Chaikoff effect: a phenomenon revealing how excessive iodine intake can reduce thyroid hormone levels. Unraveling its origins from the research of Drs. Jan Wolff and Israel Lyon Chaikoff, this effect showcases thyroid autoregulation, particularly significant in Graves’ disease management. Understand its mechanism inhibiting thyroid hormone formation and release, shedding light on iodine’s complex role in thyroid health.
Wolff-Chaikoff Effect

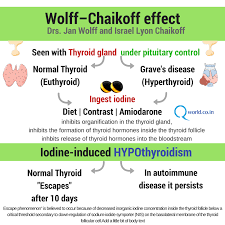
The Wolff–Chaikoff effect is the reduction in thyroid hormone levels caused by ingestion of a large amount of iodine.
It was discovered by Drs. Jan Wolff and Israel Lyon Chaikoff at the University of California, Berkeley: in 1948, they reported that injection of iodine in rats almost completely inhibited organification (thyroglobulin iodination) in the thyroid gland.12
Patients with Graves’ disease are more sensitive than euthyroid patients,3 and iodine has been used to manage Graves’ disease.
The Wolff–Chaikoff effect is known as an autoregulatory phenomenon that inhibits organification in the thyroid gland, the formation of thyroid hormones inside the thyroid follicle, and the release of thyroid hormones into the bloodstream.4 This becomes evident secondary to elevated levels of circulating iodide.

The Wolff–Chaikoff effect is an effective means of rejecting a large quantity of imbibed iodide, and therefore preventing the thyroid from synthesizing large quantities of thyroid hormone.5 Excess iodide transiently inhibits thyroid iodide organification. In individuals with a normal thyroid, the gland eventually escapes from this inhibitory effect and iodide organification resumes; however, in patients with underlying autoimmune thyroid disease, the suppressive action of high iodide may persist.6 The Wolff–Chaikoff effect lasts several days (around 10 days), after which it is followed by an “escape phenomenon,”7 which is described by resumption of normal organification of iodine and normal thyroid peroxidase function. “Escape phenomenon” is believed to occur because of decreased inorganic iodine concentration inside the thyroid follicle below a critical threshold secondary to down-regulation of sodium-iodide symporter (NIS) on the basolateral membrane of the thyroid follicular cell.

The Wolff-Chaikoff hypothyroidism is transient and thyroid function returns to normal in 2 to 3 weeks after iodide withdrawal, but transient T4 replacement therapy may be required in some patients. The patients who develop transient iodine-induced hypothyroidism must be followed long term thereafter because many will develop permanent primary hypothyroidism.
It is observed in individuals without underlying overt thyroid disorder, and especially in patients with autoimmune thyroiditis or those previously treated for thyroid.
Related Keywords:
- Thyroid health
- Hypothyroidism symptoms
- Hashimoto’s thyroiditis treatment
- Non-thyroid conditions mimicking hypothyroidism
- Thyroid function tests
- Thyroid hormone replacement therapy
Top Competitor Sites with URLs:
- EndocrineWeb – https://www.endocrineweb.com/
- American Thyroid Association – https://www.thyroid.org/
- Mayo Clinic – https://www.mayoclinic.org/diseases-conditions/hypothyroidism/
Suggested Sites for Outreach and Backlinks:
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov/
- American Association of Clinical Endocrinologists (AACE) – https://www.aace.com/
- Thyroid Foundation of Canada – https://thyroid.ca/
Footnotes
- Markou K, Georgopoulos N, Kyriazopoulou V, Vagenakis AG., Iodine-Induced hypothyroidism. Thyroid. 2001 May;11(5):501-10. ↩︎
- Lesher JL Jr, Fitch MH, Dunlap DB., Subclinical hypothyroidism during potassium iodide therapy for lymphocutaneous sporotrichosis. Cutis. 1994 Mar;53(3):128-30. ↩︎
- Wémeau JL., [Hypothyroidism related to excess iodine], Presse Med. 2002 Oct 26;31(35):1670-5. French. ↩︎
- Eng PH, Cardona GR, Previti MC, Chin WW, Braverman LE., Regulation of the sodium iodide symporter by iodide in FRTL-5 cells. Eur J Endocrinol. 2001 Feb;144(2):139-44. ↩︎
- Alexandrides T, Georgopoulos N, Yarmenitis S, Vagenakis AG., Increased sensitivity to the inhibitory effect of excess iodide on thyroid function in patients with beta-thalassemia major and iron overload and the subsequent development of hypothyroidism. Eur J Endocrinol. 2000 Sep;143(3):319-25. ↩︎
- Bando Y, Ushiogi Y, Okafuji K, Toya D, Tanaka N, Miura S., Non-autoimmune primary hypothyroidism in diabetic and non-diabetic chronic renal dysfunction. Exp Clin Endocrinol Diabetes. 2002 Nov;110(8):408-15. ↩︎
- Frey H. Hypofunction of the Thyroid Gland, Due to Prolonged and Excessive Intake of Potassium Iodide. Acta Endocrinol (Copenh). 1964 Sep;47:105-20. ↩︎
- Reinhardt W, Luster M, Rudorff KH, Heckmann C, Petrasch S, Lederbogen S, Haase R, Saller B, Reiners C, Reinwein D, Mann K. Effect of small doses of iodine on thyroid function in patients with Hashimoto’s thyroiditis residing in an area of mild iodine deficiency. ↩︎
- Panneels, V.; Juvenal, G.; Boeynaems, J.M.; Durmont, J.E.; Sande, J. Van (2009). “Iodide Effects on the Thyroid: Biochemical, Physiological, Pharmacological, and Clinical Effects of Iodide in the Thyroid”. In Preedy, Victor R.; Burrow, Gerard N.; Watson, Ronald Ross (eds.). Comprehensive Handbook of Iodine: Nutritional, Biochemical, Pathological and Therapeutic Aspects. Academic Press. p. 304. ↩︎
- Wolff J, Chaikoff IL (1948). “Plasma inorganic iodide as a homeostatic regulator of thyroid function”. J Biol Chem. 174 (2): 555–564. ↩︎
- King; Tekoa, Mary Brucker (2010). Pharmacology for Women’s Health. Jones & Bartlett Learning. p. 549. ↩︎
- Goodman, Louis Sanford; Gilman, Alfred Goodman (1996). Goodman and Gilman’s the pharmacological basis of therapeutics (9th ed.). McGraw-Hill. p. 1402. ↩︎
- Markou, K (May 2001). “Iodine induced hypothyroidism”. Thyroid. 11 (5): 501–10. ↩︎
- dennis L. Kasper, stephen L. Hauser, J. Larry Jameson, Anthony s. fauci, dan L. Longo, Joseph Loscalzo (2015). Harrison’s Principles of Internal Medicine. 19th Edition. McGraw-Hill Education. P: 2285. ↩︎
- Eng P, Cardona G, Fang S, Previti M, Alex S, Carrasco N, Chin W, Braverman L (1999). “Escape from the acute Wolff-Chaikoff effect is associated with a decrease in thyroid sodium/iodide symporter messenger ribonucleic acid and protein”. Endocrinology. 140 (8): 3404–10. ↩︎